A fundamental change in the architecture of Medicare is rapidly happening into something different to what people think the Medicare program is.
Medicare Advantage (MA) continued to grow during the pandemic, and most Medicare enrollees will be in private plans in a couple of years despite MA’s deep-rooted problems.
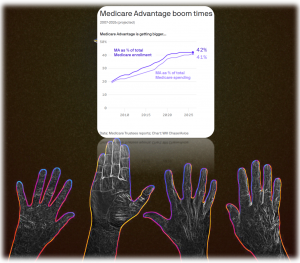
Spending on MA is rising precipitously (2021 to 2022 by over 8%) due to several policies, but the most notable is “risk adjustment.”
The Congressional Budget Office predicts MA enrollment will surpass 37 million in 2026, which would equal half of all Medicare enrollees. More individuals are picking MA plans when they turn 65, and more employers are shifting their retirees to MA plans (sometimes unknown to the retirees!)
- Numerous auditors have found insurers are overcharging the government by exaggerating how sick their members are despite the recent risk adjustment scandals
- Unlike risk adjustment in the ACA marketplaces, MA insurers get potentially unlimited funds to code as many diagnoses as possible. The risk adjustment unit for one dominant MA insurer has been known as “the office of profit planning,” according to an industry source
- MA experts argue that “The honey pot is bottomless. MA risk adjustment always goes up.”
- The giant pot of taxpayer funding is a big reason why venture capitalists have backed new insurers like Alignment Healthcare, Bright Health, Clover Health, Devoted Health and Oscar Health and why hospitals have owned MA plans
- The federal government paid almost $350B to MA insurers in 2021, a 10% increase from 2020. Every year since 2015, annual spending growth on MA plans has outpaced annual enrollment growth
- MA plans coordinate care for people within a narrower network of doctors and hospitals, but promises of saving taxpayer dollars have NOT materialized
- “No iteration of private plan contracting has yielded net aggregate savings for the Medicare program,” the Medicare Payment Advisory Commission said in its June/2021 report
MA is consuming more membership and more of the Medicare trust fund, but many enrollees are not sticking with their plans until the end. MA enrollees who are in their last year of life ditch their plans for traditional Medicare “at more than twice the rate of all other MA beneficiaries”; those people get sicker, they need more care, and their plans’ networks limit access to the doctors, hospitals, nursing homes and hospice care they want.